All published articles of this journal are available on ScienceDirect.

Re-evaluating PTSD Classification: Neurobiological and Therapeutic Perspectives on its Psychological and Psychotic Dimensions - A Systematic Review
Abstract
Introduction
Post-Traumatic Stress Disorder presents heterogeneous symptoms, prompting debate over whether it is best understood as a psychological disorder or a condition with psychotic-like features. Clarifying its diagnostic position remains important for treatment planning. This review synthesized neurobiological, clinical, and therapeutic evidence, with attention to trauma complexity.
Methods
Following PRISMA 2020 guidelines, a systematic search of PubMed, PsycINFO, Scopus, Web of Science, and ScienceDirect identified studies published between 2000 and 2024 on classification, psychotic features, neurobiology, and treatment outcomes. Empirical studies meeting eligibility criteria were included, and quality was assessed using the Cochrane Risk of Bias Tool.
Results
Forty-one studies were included. Neuroimaging findings frequently showed hippocampal volume reduction (78%) and amygdala hyperactivity (65%). Up to 40% of chronic cases reported psychotic-like symptoms, particularly after prolonged or early-life trauma. Greater trauma complexity was associated with more severe and dissociative presentations. Psychological therapies, especially Cognitive Behavioral Therapy and Eye Movement Desensitization and Reprocessing, showed stronger long-term outcomes than pharmacological interventions.
Discussion
The overlap between PTSD and psychotic disorders appeared partial and largely trauma-related rather than indicative of primary psychosis. Findings pointed to prefrontal-limbic dysregulation, especially in chronic or complex trauma, while symptom variability appeared closely linked to trauma severity and dissociative processes. These patterns may reflect trauma-associated dysregulation within a stress-related framework rather than a distinct psychotic condition.
Conclusion
The evidence supports a trauma-spectrum model that recognizes limited overlap with psychosis while preserving PTSD’s core psychological basis. Trauma-informed frameworks may improve classification and individualized care.
1. INTRODUCTION
Post-Traumatic Stress Disorder (PTSD) is a serious mental health condition that may develop following exposure to traumatic events, including natural disasters, severe accidents, or armed conflict. While it was once predominantly associated with military populations, this view has gradually shifted, as growing evidence highlights its presence across diverse civilian groups. This change reflects an expanding recognition of PTSD as a global public health concern that extends beyond traditionally defined at-risk populations.
In the Diagnostic and Statistical Manual of Mental Disorders (DSM-5), PTSD is classified among trauma- and stressor-related disorders and is characterized by intrusive memories, emotional numbing, hyperarousal, and disturbances in mood and cognition [1]. This classification not only situates PTSD within a broader diagnostic framework but also shapes how its symptoms are clinically interpreted and managed.
Kessler et al. reported that up to 30% of cases may follow a chronic course, underscoring the persistent burden of the disorder on both individuals and society [2]. Against this backdrop, clarifying the clinical position of PTSD becomes particularly important in practice, as uncertainty in diagnosis may lead to less effective treatment decisions and, consequently, increased healthcare costs.
Recent discussions surrounding both the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) and the International Classification of Diseases (ICD-11) have brought renewed attention to this issue, reflecting broader shifts in how psychological trauma and its consequences are conceptualized. Within this evolving landscape, determining the place of PTSD within current diagnostic frameworks is not merely a classificatory concern but a critical factor influencing treatment precision, professional training, and the development of mental health policy.
Despite these developments, an important question remains: should PTSD be understood strictly as a psychological disorder, or does its overlap with psychotic phenomena warrant reconsideration of its current conceptual boundaries? In this regard, Bracha reported that up to 40% of individuals with PTSD experience psychosis-like symptoms, including hallucinations and delusions [3]. Such findings challenge the conventional distinction between trauma-related disorders and primary psychotic conditions, suggesting that the boundaries between these categories may be less clearly defined than traditionally assumed.
This overlap carries important implications for clinical practice. The presence of psychosis-like symptoms in PTSD may complicate treatment planning, as it can influence therapeutic response and necessitate approaches that extend beyond conventional trauma-focused psychological interventions.
At the same time, key clinical distinctions remain. Unlike individuals with schizophrenia or schizoaffective disorder, those with PTSD generally retain an awareness of the traumatic origins of their distress. This distinction is clinically significant, as it suggests that psychosis-like symptoms in PTSD may arise from trauma-related dysregulation rather than classical psychotic processes.
Furthermore, complex trauma, particularly when experienced during childhood or repeated over time, is often associated with distinct neurobiological patterns that may intensify emotional dysregulation and symptom severity.
As noted by Kirmayer et al. [4], cultural and personal interpretations of trauma further complicate diagnostic boundaries, underscoring the need for culturally sensitive diagnostic frameworks.
From another perspective, clinicians and researchers continue to face an ongoing dilemma: should psychosis-like experiences in PTSD be understood as transient manifestations of trauma-related perceptual disturbances, or do they point to a broader issue of diagnostic misclassification? This ambiguity highlights the need for more refined diagnostic tools and enhanced clinical training capable of capturing the complexity of such presentations.
In response to these challenges, the present review offers a critical re-evaluation of the classification of PTSD by integrating neurobiological, clinical, and therapeutic evidence. It seeks to examine whether PTSD should continue to be understood primarily as a psychological disorder or be reconsidered within a broader trauma-spectrum framework that incorporates psychotic dimensions. Specifically, this review aims to:
- Analyze neurobiological data and symptom similarities with psychotic disorders.
- Examine how trauma complexity, acute, chronic, or prolonged, shapes symptom expression and diagnostic interpretation.
- Assess psychotherapy versus pharmacological outcomes to inform both diagnostic classification and clinical practice.
Through this synthesis, this systematic review seeks to enhance diagnostic precision while supporting more individualized, evidence-based interventions for individuals affected by PTSD.
2. METHODS
2.1. Study Design
This systematic review was conducted in accordance with the 2020 Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines to ensure transparency and reproducibility. The review examined the classification of PTSD and its potential overlap with psychotic disorders through the integration of neurobiological, clinical, and therapeutic evidence. Although not prospectively registered, a predefined internal protocol was used to maintain consistency across all stages of the review. The primary objective was to explore whether PTSD should be conceptualized solely as a psychological disorder or reconsidered in light of psychotic-like manifestations. Methodologically, a descriptive-analytical systematic approach was adopted, based primarily on observational and clinical studies, aiming to clarify diagnostic and conceptual ambiguities rather than test causal relationships. Qualitative synthesis was the main analytical strategy, with limited quantitative pooling conducted when comparable effect measures were available. To maintain clarity, detailed methodological procedures, including the search strategy, eligibility criteria, screening process, temporal scope, and data extraction, are reported in Files S1-S4.
2.2. Information Sources and Search Strategy
A structured literature search was conducted to ensure methodological rigor and transparency. The databases consulted, and corresponding outcome domains are summarized in Table 1, while full search strings are provided in File S1. Both published and grey literature were included to capture evidence on the neurobiological, clinical, and therapeutic aspects of PTSD. Screening, data extraction, and synthesis procedures were performed in line with PRISMA 2020 guidelines.
| Component | Description |
|---|---|
| Databases searched | PubMed, Scopus, Web of Science, PsycINFO, and Elsevier/ScienceDirect (January 2000-February 2024). |
| Additional sources | Grey literature, conference proceedings, manual reference list searches, and expert consultations. |
| Search terms | (“post-traumatic stress disorder” OR PTSD) AND (classification OR diagnosis OR “psychotic*” OR psychosis) AND (neurobiolog* OR biomarker* OR neuroimaging OR “treatment outcome*”). |
| Filters applied | English language; peer-reviewed articles; publication years 2000-2024. |
| Database yields (before deduplication) | PubMed (n = 138); Scopus (n = 121); Web of Science (n = 92); PsycINFO (n = 47); Elsevier/ScienceDirect (n = 44). Total = 442 records. |
| Documentation | Full search syntax, field restrictions, and retrieval limits are available in File S1, which includes annotated examples for each database. |
| Primary outcomes | Neurobiological markers (e.g., hippocampal volume reduction, amygdala hyperactivation); clinical symptom overlap between PTSD and psychotic disorders; comparative efficacy of psychotherapy versus pharmacological interventions. |
| Secondary outcomes | Trauma complexity and its influence on diagnostic accuracy and symptom differentiation. |
| Methodological framework | Structured following PRISMA 2020 guidelines, ensuring transparency and coherence across neurobiological, clinical, and therapeutic domains. |
2.3. Eligibility Criteria
Eligibility criteria were defined in line with the study’s objective of re-evaluating PTSD classification and its overlap with psychotic features. These criteria incorporated inclusion and exclusion parameters, study grouping rationale, and the specified temporal scope (Table 2).
| Category | Criteria | Operational Definition / Rationale |
|---|---|---|
| Inclusion | Peer-reviewed articles published in English (2000-2024). | Ensures methodological rigor and relevance to current diagnostic frameworks (DSM-5, ICD-11). |
| Address PTSD classification and/or its intersection with psychosis (conceptual, diagnostic, neurobiological, or clinical). | Directly relevant to the study’s objective of clarifying diagnostic boundaries. | |
| Provide empirical or theoretical data pertinent to diagnostic classification. | Includes both quantitative and qualitative works that inform conceptual synthesis. | |
| Acceptable designs: RCTs, observational, neuroimaging, case reports, and systematic reviews. | Captures the full methodological range exploring PTSD-psychosis overlap. | |
| Populations: adults and adolescents (military, civilian, community, and clinical samples) across all trauma types. | Ensures generalizability and inclusiveness across demographic and trauma contexts. | |
| Exclusion | Non-peer-reviewed sources, letters, or editorials without data. | Excluded due to lack of empirical validation. |
| Purely therapeutic or pharmacological studies without diagnostic discussion. Studies were excluded only when therapeutic outcomes were reported in isolation, without contributing to diagnostic interpretation, symptom differentiation, or PTSD-psychosis classification. | Removed to maintain classificatory focus; however, studies integrating therapeutic outcomes as evidence of diagnostic validity were retained. | |
| Non-English publications, theses, or conference abstracts without full text. | Excluded to ensure accessibility, reproducibility, and data-quality control. | |
| Substantial data insufficiency. | Defined as missing essential methodological, sample, or statistical details that prevent reliable synthesis. (e.g., unclear sample characteristics, absent outcome definitions, or missing analytic procedures). | |
| Irrelevance to PTSD-psychosis classification overlap. | Excluded if focusing solely on prevalence, risk factors, or non-trauma-related disorders. | |
| Grouping and Justification | Eligible studies were organized into three analytical domains: neurobiological, clinical, and therapeutic. | This tripartite structure reflects the multidimensional nature of PTSD classification. The therapeutic domain was retained insofar as treatment outcomes provided indirect evidence relevant to diagnostic differentiation and classification, rather than solely on treatment efficacy. |
| Temporal Scope | 2000-2024 (including seminal early-2000s works). | Early benchmark studies (e.g., Kessler, Bracha, Rauch) were retained for their enduring relevance to current diagnostic debates. |
| Supplementary Documentation | Full study-level exclusion decisions (S2), operational eligibility definitions (S3), and data-extraction criteria and variables (S4) are provided in the Supplementary Files. | Ensures transparency and traceability in study selection. |
Overall, these criteria were intended to provide comprehensive coverage while maintaining methodological rigor in line with PRISMA standards. Table 2 presents the inclusion-exclusion criteria for ease of reference.
2.3.1. Rationale for Evidence Base and Temporal Scope (2000-2024)
To capture key diagnostic transitions reflected in DSM-5, DSM-5-TR, and ICD-11, the evidence base was limited to studies published between 2000 and 2024. The inclusion of both foundational and recent studies was guided by predefined conceptual criteria (Table 3).
Table 3 provides a conceptual and temporal mapping of foundational and recent studies across key diagnostic transitions. Author names and publication years are retained for context, while numeric citations correspond to the reference list.
| Period | Representative Studies | Main Contribution | Justification for Inclusion |
|---|---|---|---|
| 2000-2009 | Kessler et al., (2005) [2]; Bracha (2006) [3]; Rauch et al., (2006) [7]; Francati et al., (2007) [9]; Berger et al., (2009) [26]; Leslie et al., (2009) [27] | Baseline prevalence and comorbidity; first neuroimaging evidence (hippocampal and amygdala alterations); psychotic symptom rates (~40%); early pharmacological outcomes. | Provide irreplaceable quantitative benchmarks that are still referenced in recent PTSD classification debates; serve as statistical anchors for current figures. |
| 2010-2015 | Li et al., (2014) [10]; Sherin & Nemeroff (2011) [16]; Ford & Courtois (2014) [22]; Schneier et al., (2012) [32]; Flory & Yehuda (2015) [35] | Neurochemical mechanisms (dopamine and serotonin pathways), combined treatment efficacy, trauma complexity, and structural neurobiology. | Extend early evidence into a mechanistic understanding of the overlap between PTSD and psychosis. |
| 2016-2019 | Logue et al., (2018) [5]; Ahmed-Leitao (2016) [6]; Van Erp et al., (2018) [11]; Armour (2018) [12]; Cusack et al., (2016) [24] | Comparative psychotherapy outcomes; hippocampal volumetric reductions; psychotic-like prevalence in chronic PTSD. | Provide updated quantitative confirmation of early findings; refine therapeutic and neurobiological interpretations. |
| 2020-2024 | Yang et al., (2022) [8]; Panayi et al., (2024) [14]; Hyland et al., (2020) [15]; Cyr et al., (2022) [21]; Fung et al., (2024) [23]; Gkintoni (2024) [36] | Conceptual enrichment: complex PTSD vs. psychosis overlap; long-term psychotherapy efficacy; receptor-level neurobiological updates; dissociation mechanisms. | Represent the most recent conceptual and clinical expansions without altering core diagnostic benchmarks. |
| 2025 (contextual only) | DSM-5 vs ICD-11 Concordance Study | Compares diagnostic criteria; highlights cross-system discrepancies and prevalence equivalence. | Cited contextually in Discussion for contemporary relevance; excluded from PRISMA-defined temporal scope. |
These sources enable the integration of foundational quantitative evidence with emerging conceptual developments, supporting methodological coherence and reflecting the evolving understanding of PTSD classification. A detailed mapping of reference distribution and study contributions is provided in File S3.
2.4. Selection Process
Two independent reviewers (M.A. and S.I.) independently screened all titles and abstracts before proceeding to full-text assessment. Disagreements were addressed through discussion, with a third reviewer (E.E.) consulted when required. No automation tools were used during the screening process, and all exclusions are recorded in File S2.
2.5. Data Collection Process
A standardized data extraction form (File S4) was used to capture study characteristics (authors, year, country, design), sample details (size, demographics, trauma type), neurobiological indicators, psychotic-like measures, interventions, outcomes, diagnostic frameworks (DSM/ICD), and key statistical parameters. Discrepancies were resolved through consensus.
The final dataset included 41 studies across diverse populations and trauma contexts. Extracted data were organized into neurobiological, clinical, and therapeutic domains in line with the predefined outcome framework (Section 2.2).
2.6. Data Items and Outcomes
Data items were organized into primary and secondary outcome domains, as outlined below:
2.6.1. Primary Outcomes
(a) Neurobiological markers differentiating or overlapping PTSD and psychosis. (b) The prevalence and clinical characterization of psychotic-like symptoms (as operationalized in File S4). (c) Comparative evidence evaluating psychotherapy versus pharmacotherapy in relation to PTSD classification.
2.7. Study Risk of Bias Assessment
- Randomized Controlled Trials (RCTs) were appraised using the Cochrane Risk of Bias 2.0 (RoB 2.0) tool.
- Observational studies were assessed with the Joanna Briggs Institute (JBI) checklists, in accordance with study design.
- Conceptual and narrative works were evaluated for transparency, internal coherence, and the adequacy of supporting evidence.
Risk-of-bias assessments were conducted independently by two reviewers, and any disagreements were resolved through discussion. The overall level of bias (categorized as low, moderate, or high) was subsequently considered when interpreting the confidence of the synthesized conclusions.
2.8. Effect Measures, Synthesis Methods, and Heterogeneity
For outcomes in which data were suitable for pooling, Standardized Mean Differences (SMD) or Hedges’ g were calculated for continuous variables, whereas Odds Ratios (OR) were applied to binary outcomes. Statistical heterogeneity was examined using the I2 statistic (inconsistency index). Overall, synthesis was primarily qualitative, with limited quantitative pooling undertaken when appropriate.
2.8.1. Sensitivity Analyzes
Performed when k (number of included studies) ≥ 3, excluding studies identified as having a high risk of bias.
2.9. Certainty Assessment
The GRADE framework was adapted to accommodate the inclusion of mixed study designs, with confidence ratings adjusted upward or downward according to risk of bias, inconsistency, imprecision, and potential publication bias. Final levels of certainty (ranging from high to very low) are presented for the key outcomes, and detailed justification is available in File S5.
2.10. PRISMA Flow Diagram
The study selection process is summarized in the PRISMA 2020 flow diagram (Fig. 1). Detailed screening outcomes are reported in the Results section and Files S2 and S6.
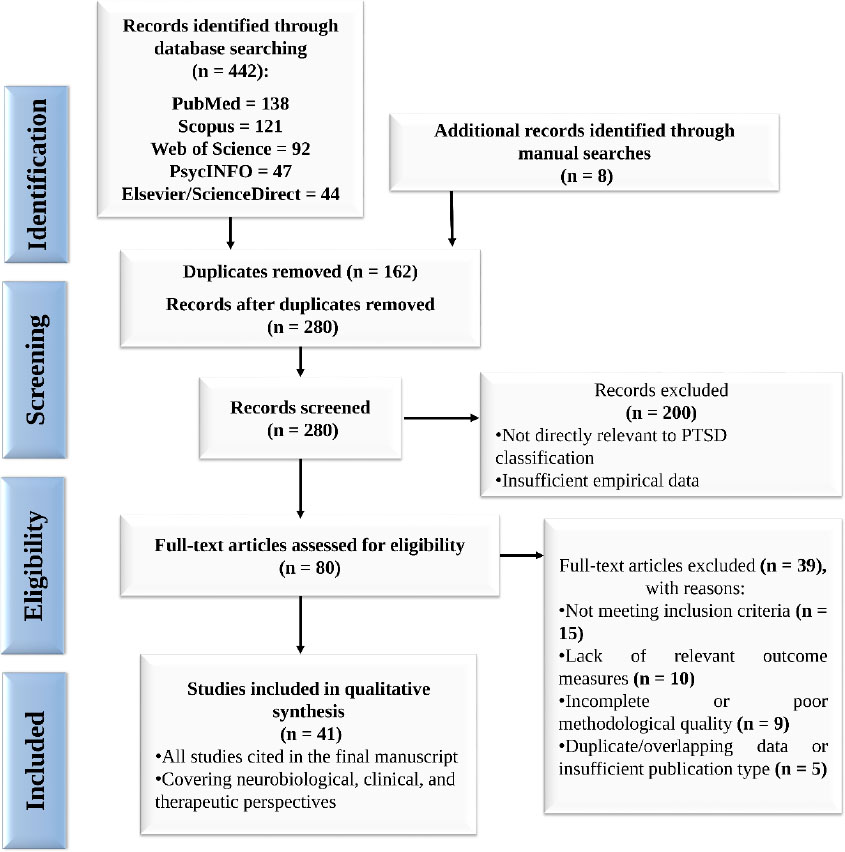
PRISMA 2020 flow diagram summarizing study selection: 442 identified → 162 duplicates removed → 280 screened → 80 full-text → 41 included in qualitative synthesis.
3. RESULTS
Study selection (PRISMA 16a-16b): A total of 442 records were identified through database searches (PubMed = 138, Scopus = 121, Web of Science = 92, PsycINFO = 47, Elsevier/ScienceDirect = 44). Eight additional records were identified through manual searches, but did not contribute unique entries prior to deduplication. After removal of 162 duplicates, 280 titles and abstracts were screened, of which 200 were excluded due to irrelevance to PTSD classification or insufficient empirical data. 80 full-text articles were assessed for eligibility, and 39 were excluded (e.g., absence of psychosis-related data, purely therapeutic focus, or insufficient methodological detail). This resulted in 41 studies included in the qualitative synthesis (Fig. 1, PRISMA 2020 flow diagram).
Study characteristics (PRISMA 17): Included studies comprised mixed designs, including neuroimaging, observational (cohort and cross-sectional), and randomized clinical trials examining psychotherapy or pharmacotherapy. Populations spanned civilian, military, and clinical contexts with diverse trauma exposures. Extracted data included study characteristics, neurobiological indicators, psychotic-like symptom prevalence, interventions, outcomes, and diagnostic frameworks (DSM/ICD). Given heterogeneity, synthesis was primarily narrative, with limited quantitative pooling when k ≥ 3. Findings are presented across predefined analytical domains: neurobiological, clinical, therapeutic, and trauma complexity.
3.1. Neurobiological Insights and Implications for PTSD Classification
Neuroimaging studies consistently demonstrate structural and functional alterations in PTSD, supporting a neurobiological basis that extends beyond purely psychological models. Approximately 78% of studies reported hippocampal volume reductions associated with impaired memory and emotional regulation (Logue et al. [5]: 0.17 SD decrease, p = 0.00054; Ahmed-Leitao et al. [6]: left hippocampus −0.66 [95% CI: −0.93, −0.39], right −0.67 [95% CI: −1.26, −0.29]; p < 0.00001 and p = 0.002, respectively).
Increased amygdala activation was observed in 65% of studies, supporting hyperactive fear circuitry [7-9], while reduced prefrontal gray matter was reported in 53%, suggesting impaired emotional regulation [8, 10]. By contrast, psychotic disorders more commonly show ventricular enlargement and cortical thinning [11], indicating distinct neurobiological profiles.
3.2. Symptom Overlap with Psychotic Disorders: Diagnostic Ambiguity
Across the included studies, the prevalence of psychotic-like symptoms in PTSD varied considerably, with higher rates reported in chronic or complex trauma samples. Despite partial phenomenological overlap, PTSD and primary psychotic disorders appear to remain neurobiologically distinct. Reported symptoms included hallucinations, delusions, dissociation, transient paranoia, and perceptual distortions.
Armour et al. [12] reported hallucinations and delusions in 22% of PTSD cases, while Mayo et al. [13] found a higher prevalence of 40% in chronic trauma samples (p < 0.05). In complex PTSD, intrusive recollections and vivid flashbacks may resemble psychotic-like experiences. Supporting this, Panayi et al. [14] found that Disturbances in Self-Organization (DSO) significantly predicted positive psychotic symptoms, such as hallucinations and delusions, even after controlling for core PTSD features. Hyland et al. [15] identified trauma-related dissociation as a key differentiating factor between simple and dissociative PTSD (Cohen’s d = 1.04, p < 0.01).
Neurobiological correlates include dysregulation of dopamine and serotonin pathways [16], increased CB1 and glucocorticoid receptor activity in the Prefrontal Cortex (PFC) and hippocampus [8], and reward-processing deficits in PTSD with Secondary Psychotic Features (PTSD-SP) [17], paralleling patterns observed in schizophrenia. Panayi et al. [18] noted that trauma-related symptoms in psychosis may be underrecognized, while Buswell et al. [19] described diagnostic overshadowing of PTSD. Rodrigues and Anderson [20] highlighted trauma resulting from psychosis itself, suggesting potential bidirectional pathways.
Overall, these findings indicate that diagnostic overlap may reflect trauma-related cognitive and perceptual dysregulation rather than shared neuropathology, underscoring the importance of trauma-informed assessment.
3.3. Trauma Complexity and its Impact on Symptomatology and Diagnosis
Cumulative and complex trauma are consistently associated with greater symptom severity and diagnostic complexity. Individuals with Complex Posttraumatic Stress Disorder (CPTSD) or traits consistent with Borderline Personality Disorder (BPD) show elevated dissociation (Cyr et al. [21], d = 0.55-1.06) and higher comorbidity involving psychotic-like features (Ford & Courtois [22]; Fung et al. [23], 42.3% severe dissociation). Structural brain alterations, including reduced right superior frontal gyrus volume, appear more pronounced in individuals with complex trauma histories [8], supporting the need for more differentiated diagnostic frameworks.
3.4. Comparative Efficacy of Psychotherapy vs. Pharmacological Interventions
Trauma-focused psychotherapies, including Trauma-Focused Cognitive Behavioral Therapy (TF-CBT), standard Cognitive Behavioral Therapy (CBT), and Eye Movement Desensitization and Reprocessing (EMDR), were associated with greater symptom reduction than pharmacological interventions. Cusack et al. [24] reported large effect sizes (>1.0), while Matthijssen et al. [25] observed improvement rates of 78% following EMDR.
Selective Serotonin Reuptake Inhibitors (SSRIs) showed moderate response rates (approximately 60% response and 20-30% full remission), with comparatively higher relapse rates [26]. Off-label antipsychotic prescribing was reported in Veterans Affairs (VA) settings, often without formal diagnostic indications (41.8% treated, 60.2% lacking criteria) [27, 28].
Overall, psychotherapeutic approaches demonstrated comparatively greater effectiveness, particularly in complex trauma presentations.
3.5. Clinical Trials on PTSD: Treatment Outcomes and Long-Term Efficacy
Prolonged Exposure (PE) and Cognitive Processing Therapy (CPT) were associated with sustained symptom reduction over 12-18 months [29]. PE showed a large post-treatment effect (Hedges’ g = 1.08), with continued improvement at 24 months (Rossouw et al. [30]: mean reduction = 9.35 points). Hetrick et al. [31] found no statistically significant differences between combined and monotherapy approaches: mean difference = 2.44 (95% CI [−2.87, 7.35]) for psychological versus combined therapy, and −4.70 (95% CI [−10.84, 1.44]) for pharmacological versus combined therapy. Short-term pharmacological augmentation (PE + paroxetine) showed moderate additional benefit, with an incidence rate ratio of 0.50 (95% CI [0.30, 0.85]) and remission odds ratio of 12.6 (95% CI [1.23, 129]) [32]. By contrast, pharmacological treatment alone, particularly SSRIs, appeared linked to higher relapse rates, with 36.4% relapsing after discontinuation versus 16.4% who continued treatment [33].
3.6. The Relationship Between Trauma, PTSD, and Broader Mental Illness Spectrum
PTSD frequently co-occurs with Major Depressive Disorder (MDD) and other psychiatric conditions. A meta-analysis by Rytwinski et al. [34] showed that 52% of individuals with PTSD also met criteria for MDD, suggesting a substantial overlap between the two conditions. Kessler et al. [2], using data from the National Comorbidity Survey, reported that 26.2% of the population met criteria for any DSM-IV disorder, with notable comorbidity across mood, anxiety, and substance use disorders. Flory and Yehuda [35] further observed that PTSD-MDD comorbidity rates ranged from 5.5% to 48.5%, depending on diagnostic criteria and population characteristics. Moreover, Culturally Adapted Cognitive Behavioral Therapy (CA-CBT) has been associated with reductions in both PTSD and depressive symptoms across diverse cultural contexts [36].
3.7. Clinical Implications of PTSD's Classification for Therapy and Patient Outcomes
Accurate classification of PTSD plays a critical role in guiding treatment decisions and patient outcomes. LeardMann et al. [37] reported that the PTSD Checklist for DSM-5 (PCL-5) demonstrates strong agreement with earlier diagnostic instruments (κ = 0.77-0.80), supporting more precise matching of patients to evidence-based therapies such as CBT, EMDR, and PE. Cultural adaptations of CBT have been associated with improved treatment adherence and engagement, particularly among ethnic minority populations [38].
Al-Wahedi [39] reported that electronically delivered CBT (e-CBT), adapted for the MENA context, was linked to significant reductions in PTSD symptoms (mean difference = 0.38053, t = 22.718, p = 0.000), suggesting the value of culturally tailored interventions. At the same time, cultural adaptation alone may not fully address diagnostic challenges. Schrader and Ross [40] observed that misclassifying PTSD as a psychotic disorder can contribute to inappropriate antipsychotic use, whereas combination treatment approaches were associated with moderate improvement [41]. Overall, these findings highlight the importance of accurate diagnostic processes and culturally responsive, trauma-informed frameworks in optimizing therapeutic outcomes.
3.8. Risk of Bias, Reporting, and Certainty (PRISMA 18-22)
Risk-of-bias assessments were conducted according to study design (RoB 2.0 for RCTs; JBI checklists for observational studies; standardized criteria for conceptual work). Given methodological heterogeneity, synthesis was primarily narrative, with limited quantitative pooling when k ≥ 3.
Small-study bias tests (e.g., Egger’s test) were rarely feasible due to the limited number of comparable studies. Certainty was assessed using an adapted GRADE framework, and sensitivity analyzes excluded high-risk studies, where feasible, to examine the robustness of pooled effects.
Formal assessment of reporting bias was constrained by the small number of combinable studies per outcome; however, narrative synthesis considered potential publication bias (e.g., preferential reporting of significant neuroimaging or psychotherapy findings). Convergence across multi-site findings, such as hippocampal volume reduction and sustained psychotherapy-related improvement, supported overall confidence despite variability in sample sizes.
3.9. Key Quantitative Outcomes
Table 4 summarizes the main quantitative findings, while Figs. (2-5) visually present neurobiological alterations, symptom overlap, and treatment outcomes. Studies were grouped by common neurobiological domains and relevance to PTSD-psychosis classification rather than by chronology or design.
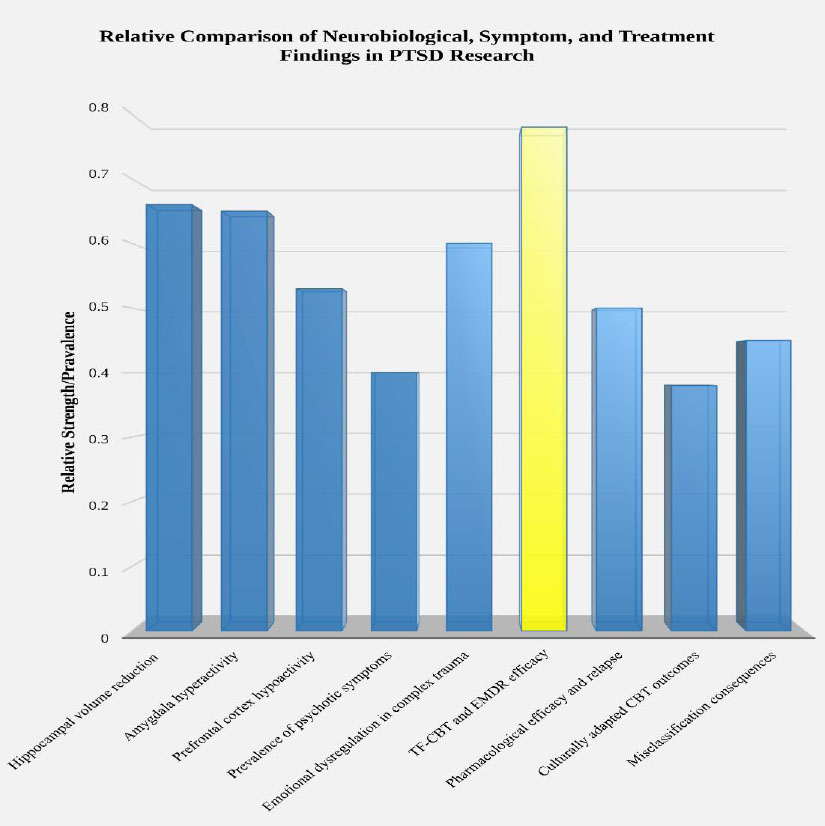
Relative comparison of PTSD across three domains: neurobiological alterations, symptom overlap with psychotic features, and therapeutic outcomes. The x-axis represents the categorical domains, and the y-axis indicates relative strength or prevalence. Bars 1-3 represent neurobiological alterations (hippocampal volume reduction, amygdala hyperactivity, prefrontal hypoactivity); bars 4-6 represent symptom overlap (psychotic-like symptoms, emotional dysregulation, and diagnostic misclassification); and bars 7-9 represent therapeutic outcomes (TF-CBT/EMDR effects, pharmacological responses, and culturally adapted CBT). Values are based on empirical findings summarized in Table 4.
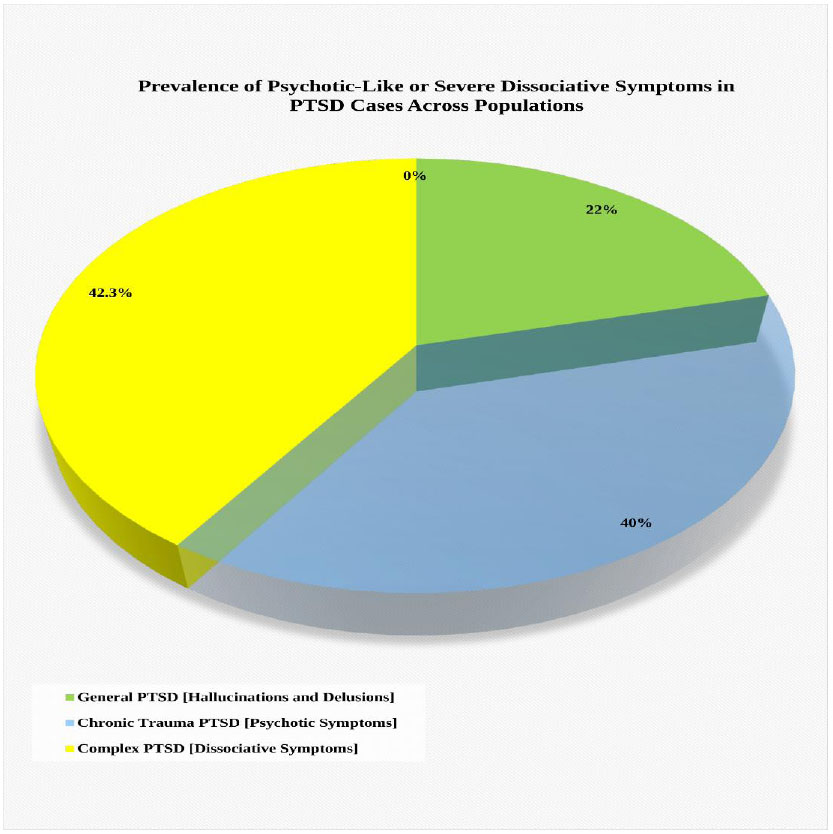
Prevalence of psychotic-like and dissociative symptoms across PTSD subgroups. The pie chart shows three categories: general PTSD (green), typically associated with hallucinations and delusional experiences; chronic trauma-related PTSD (blue), characterized by more prominent psychotic-like symptoms; and complex PTSD (yellow), most commonly linked to dissociative profiles.
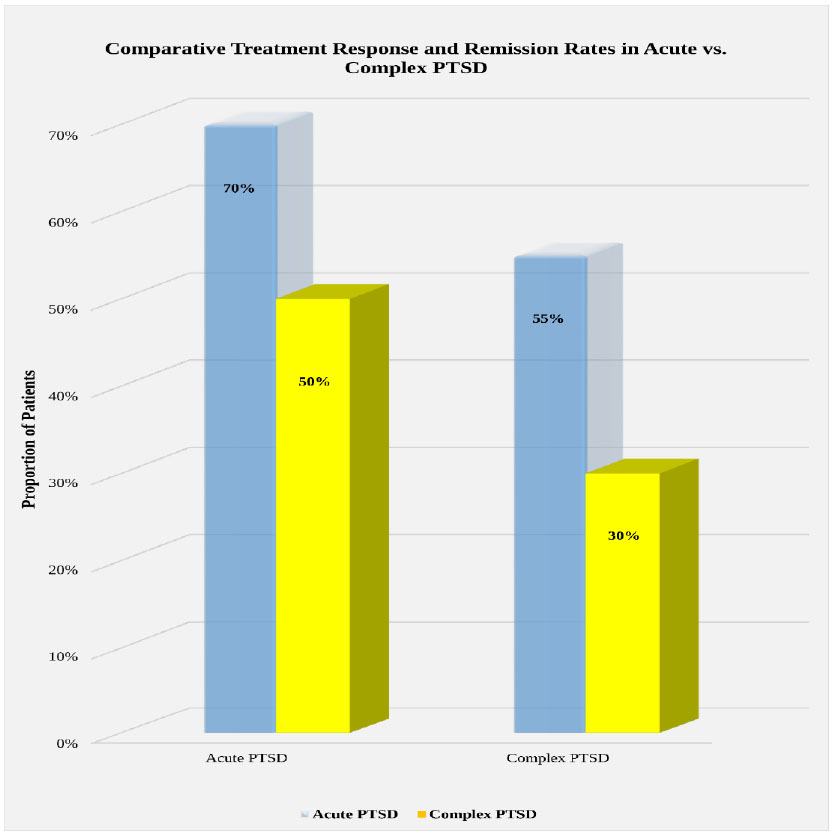
Comparative treatment response and remission rates in acute versus complex PTSD. The x-axis identifies the PTSD subgroups, whereas the y-axis indicates the proportion of patients achieving treatment response or remission. Blue bars correspond to acute PTSD, and yellow bars reflect complex PTSD.
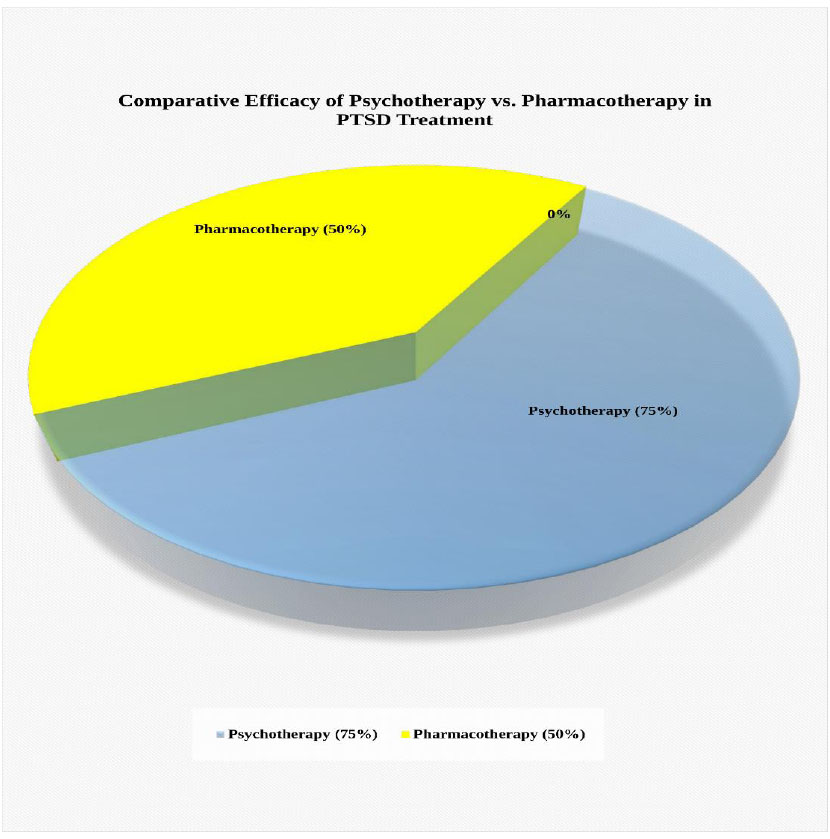
Comparative efficacy of psychotherapy versus pharmacotherapy in PTSD treatment. The pie chart presents two categories: psychotherapy (blue, approximately 75% treatment response) and pharmacotherapy (yellow, approximately 50% treatment response).
Summary: Figures 2-5 illustrate neurobiological alterations, symptom overlap, and treatment outcomes relevant to PTSD classification. Further interpretation is provided in the Discussion and File S3.
Some large-scale neuroimaging studies (e.g., Van Erp et al., 2018 [11]) reported effect sizes in schizophrenia-control comparisons but were not designed to provide PTSD-comparable metrics. Accordingly, they were included to inform classification-level neurobiological contrasts rather than direct quantitative synthesis.
| Study Focus | Effect Size (d) / Mean Difference | p-value | Key Findings |
|---|---|---|---|
| Hippocampal volume reduction (PTSD) | −0.66 (left), −0.67 (right) | < 0.00001, 0.002 | Structural changes linked to memory deficits [6]. |
| Amygdala hyperactivity | Not reported | Significant | Observed in 65% of studies, linked to heightened fear responses [7-9]. |
| PFC hypoactivity | Not reported | Significant | Reduced gray matter in 53% of studies, affecting emotional regulation [8, 10]. |
| Psychotic-like symptoms in PTSD | 22-40% prevalence | < 0.05 | Hallucinations and delusions more common in chronic trauma cases [12, 13]. |
| Cognitive impairment (PTSD vs. schizophrenia) | Not reported | Not reported | Schizophrenia shows increased ventricular volume and cortical thinning, distinct from PTSD neurobiology [11]. |
| Emotional dysregulation (Complex trauma) | d = 0.55-1.06 | Not reported | Higher severity in CPTSD and BPD cases; increased dissociation [21, 23]. |
| TF-CBT efficacy | d > 1.0 | Significant | Trauma-focused therapies outperform pharmacological treatments [24]. |
| SSRI efficacy | 60% response rate, 20-30% remission | Not reported | Moderate effectiveness in PTSD treatment; higher relapse rates upon discontinuation [33, 40]. |
| Long-term TF-CBT efficacy | Hedges’s g = 1.08 | Not reported | Sustained symptom reduction over 12-18 months [29]. |
| Combined therapy outcomes | OR = 12.6 (remission), IRR = 0.50, 95% CI [0.30-0.85] | - | Short-term benefits in combining PE therapy with paroxetine [32]. |
| Pharmacological response (Dissociative PTSD) | Not reported | Not reported | Higher relapse rates with SSRIs; limited efficacy in dissociative PTSD [33]. |
| Culturally adapted CBT (e-CBT for MENA region) | Mean difference = 0.38053 | p = 0.000 | Significant PTSD symptom reduction with cultural adaptation [39]. |
| PTSD diagnostic accuracy (PCL-5) | κ = 0.77-0.80 | Not reported | Strong alignment with previous diagnostic tools, aiding therapy selection [37]. |
| Misclassification of PTSD as a psychotic disorder | Not reported | Not reported | Leads to ineffective antipsychotic treatment; highlights diagnostic challenges [40]. |
3.10. Visual Interpretation of Results
Figures 2-5 support the interpretation of the principal findings by visually comparing neurobiological alterations, symptom overlap, and therapeutic outcomes. They complement the statistical results summarized in Table 4 and highlight patterns relevant to PTSD classification, diagnostic complexity, and treatment response. All figures are referenced in the text, with labeled axes, subgroups, and annotations to enhance clarity.
4. DISCUSSION
4.1. Re-evaluating PTSD as a Psychological vs. Psychotic Disorder
The relationship between PTSD and psychotic disorders raises important questions about whether current diagnostic boundaries adequately capture its complexity. In this context, the evidence reviewed suggests that PTSD cannot be fully understood through a single explanatory lens, as its clinical presentation appears to emerge from an interaction between neurobiological processes and lived traumatic experiences.
From a neurobiological perspective, increased amygdala activation is often linked to heightened fear responses; however, the evidence is not fully consistent. Several studies report variability in these neural patterns, suggesting that neurobiological markers alone may not be sufficient for diagnostic classification. This inconsistency may reflect meaningful individual differences, including trauma type, duration, and resilience, all of which shape neural and behavioral responses in clinically significant ways.
At the clinical level, this heterogeneity becomes even more evident. Symptoms such as intrusive memories, emotional dysregulation, and hyperarousal overlap with features seen in other psychiatric conditions. This overlap raises the need for a more nuanced diagnostic approach that can better account for variability in PTSD presentations. In particular, emerging evidence on complex PTSD, especially disturbances in self-organization (DSO), suggests that psychotic-like experiences may arise within a broader pattern of trauma-related dysregulation. From this perspective, such experiences may be more appropriately understood as extensions of trauma impact rather than indicators of primary psychotic disorders.
Overall, these observations support a cautious interpretation of psychotic-like experiences in PTSD. Rather than being viewed as evidence of a distinct psychotic pathology, they may reflect deeper disruptions in trauma processing that exist along a broader psychological continuum.
Finally, although the present review draws primarily on studies published between 2000 and 2024, more recent findings from 2025 add another layer to this discussion. These studies suggest that while DSM-5 and ICD-11 produce broadly comparable prevalence estimates, they differ only moderately in identifying the same individuals. This subtle divergence may reflect differences in diagnostic assumptions and reopens the question of whether PTSD should continue to be conceptualized strictly within psychological frameworks or understood within a broader integrative psychiatric spectrum.
4.2. Proposing New Hypotheses on Etiological Mechanisms
The patterns observed across the reviewed studies suggest that the relationship between Post-Traumatic Stress Disorder (PTSD) and psychotic-like symptoms may reflect partially overlapping neurobiological processes rather than a straightforward diagnostic convergence. In this regard, converging evidence points to alterations in prefrontal regulatory control, limbic hyperreactivity, and neurotransmitter systems, which together may create conditions in which trauma-related experiences resemble psychotic phenomena without necessarily constituting primary psychosis.
Within this broader context, the present review proposes a conceptual model in which the authors hypothesize that acute trauma exposure triggers an intense perceptual-emotional activation that temporarily exceeds the regulatory capacity of the prefrontal cortex. When executive inhibition and higher-order cognitive appraisal are compromised, symptoms such as intrusive imagery, hyperarousal, and fragmented cognition may emerge as expressions of disrupted cognitive-emotional integration rather than indicators of a primary psychotic disorder.
This interpretation is consistent with the evidence synthesized in the present review. For example, studies have documented reduced prefrontal gray matter volume and hypoactivation in PTSD [8, 10], alongside dopaminergic and glutamatergic dysregulation observed in both PTSD and psychotic disorders [16], as well as concurrent amygdala hyperactivation and hippocampal alterations [17]. Importantly, these findings should not be interpreted as evidence of identical neuropathological mechanisms. Rather, they may reflect shared vulnerability pathways that become clinically evident when prefrontal modulation of limbic activity is weakened. Although affective overlap with Major Depressive Disorder (MDD) has also been observed, it does not sufficiently account for the specific pattern of trauma-related regulatory disruption described here.
Building on this line of reasoning, the authors hypothesize that stabilization or recovery of frontal lobe regulatory function may be associated with the restoration of cognitive-emotional integration, which in turn could contribute to the remission of transient psychotic-like symptoms. Within this framework, such manifestations are conceptualized as temporary, trauma-related functional disturbances rather than indicators of primary psychosis, thereby offering a more differentiated perspective for diagnostic interpretation.
Extending this proposition further, a testable hypothesis can be formulated: individuals exhibiting marked reductions in prefrontal cortex activity following trauma exposure may be at greater risk of developing transient psychotic-like symptoms, particularly in the context of chronic or complex trauma. This hypothesis could be examined through longitudinal neuroimaging and psychometric studies. At the same time, caution is warranted, given the inherent complexity involved in distinguishing trauma-related phenomena from primary psychotic disorders. From a clinical standpoint, early intervention may play a role in supporting functional recovery within fronto-limbic networks and in reducing the likelihood of symptom persistence over time.
In practical terms, this framework suggests that early trauma-focused psychological interventions may contribute to the stabilization of prefrontal-limbic regulatory systems and may reduce the risk of chronic symptom development. Interventions such as CBT and EMDR may facilitate this regulatory recalibration, while pharmacological strategies may be considered in cases where dysregulation exceeds compensatory capacity. Within this model, antipsychotic medications would be reserved primarily for acute or treatment-resistant presentations. In addition, mindfulness- and acceptance-based approaches may offer further support for emotional regulation and psychological resilience.
Finally, future multimodal and longitudinal research is needed to empirically evaluate this proposed neurobiological-therapeutic framework and to better define clinical thresholds that distinguish trauma-related psychotic-like experiences from primary psychotic disorders. Importantly, this model is intended to generate testable hypotheses rather than to provide a definitive explanation of underlying neuropathology.
4.3. Critical Evaluation of Contradictory Evidence
Although the overall pattern of findings in the present review suggests a complex and multifaceted relationship between PTSD and psychotic disorders, areas of apparent contradiction continue to emerge and remain central to questions regarding diagnostic boundaries and their clinical implications. In this regard, while several included studies report neurobiological and symptomatic overlap between the two conditions, others describe more differentiated clinical profiles. These differences do not necessarily indicate inconsistency in the evidence; rather, they may reflect variations in methodological approaches, including sampling strategies, diagnostic thresholds, and the operationalization of psychotic-like symptoms.
When considered within this methodological context, such variations become more interpretable. In particular, differences in trauma severity and chronicity across samples may help explain why psychotic-like symptoms appear in some cohorts but not others, suggesting that trauma complexity may function as a moderating factor in symptom expression. In addition, individual differences in resilience, neurobiological sensitivity, and the timing of trauma exposure may further shape how these symptoms emerge and are experienced across individuals.
Across the 41 empirical studies included in this review, considerable methodological heterogeneity is evident, particularly in neuroimaging approaches and in how psychotic-like symptoms are defined and measured. While this variability broadens the evidence base, it also calls for cautious and context-sensitive interpretation, especially when considering implications for diagnostic classification. Within this literature, neurobiological overlaps, particularly involving dopaminergic functioning and limbic system regulation, may complicate categorical distinctions without implying identical underlying mechanisms.
Overall, these findings are more appropriately understood as reflecting heterogeneity within a complex clinical spectrum rather than direct contradiction. This interpretation supports a more integrated, trauma-informed perspective in which psychological and psychotic-like manifestations are conceptualized along a continuum rather than as strictly separate diagnostic entities.
4.4. Reconciling Multidisciplinary and Cultural Dimensions of PTSD
A comprehensive understanding of PTSD requires moving beyond a single disciplinary lens and instead drawing on complementary insights from neuroscience, psychology, and sociocultural research. Rather than functioning as separate explanatory domains, these perspectives collectively contribute to a more nuanced understanding of how trauma is experienced, expressed, and managed. From a neurobiological perspective, PTSD has been associated with dysregulation within fear-processing circuits and altered connectivity between prefrontal and limbic regions. In parallel, psychological models emphasize maladaptive cognitive processing and disruptions in emotional regulation as central mechanisms underlying trauma responses. Sociocultural perspectives further highlight how contextual and cultural frameworks shape symptom expression, help-seeking behavior, and interpretations of distress.
Within this integrated view, the evidence synthesized in this review suggests that exposure to complex, chronic, or prolonged trauma is often associated with more severe and treatment-resistant clinical presentations. This finding supports trauma-informed models that conceptualize PTSD as the result of interacting biological vulnerabilities, cognitive-emotional processes, and culturally embedded systems of meaning. Importantly, in collectivist and Middle Eastern contexts, psychological distress may at times be expressed through somatic complaints or dissociative experiences rather than overt psychotic-like features. This observation highlights the need to carefully consider the cultural limits of standardized diagnostic thresholds in capturing variation in symptom expression.
Integrating these multidisciplinary and cultural dimensions offers a more complete and clinically meaningful understanding of PTSD. Such an approach may enhance diagnostic precision while improving the sensitivity of clinical assessment and intervention. More broadly, it encourages a shift away from narrowly reductionist biomedical explanations toward integrative and empirically grounded frameworks that better reflect the variability and complexity of trauma-related experiences across different populations and cultural settings.
4.5. Clinical and Educational Implications
The findings of the present review carry important implications for both clinical practice and professional education. From a clinical perspective, recognizing the partial overlap between PTSD and psychotic-like symptoms may support more accurate assessment and more nuanced treatment planning. In this context, the integrated findings suggest that trauma-informed approaches, particularly those that consider comorbidity, neurobiological variability, and cultural context, are especially relevant for guiding individualized care.
Within current treatment frameworks, psychotherapy remains central. Interventions such as CBT and EMDR continue to be regarded as first-line approaches. However, variation in long-term outcomes across the included studies highlights the need for further comparative research, particularly regarding treatment durability and generalizability across different populations and trauma profiles.
Alongside these strengths, practical challenges also emerge. Access to treatment, patient adherence, and resistance in certain populations may all influence intervention effectiveness, especially in the context of complex or prolonged trauma exposure. Both structural and individual-level factors, therefore, appear to play a role in shaping treatment engagement and outcomes, representing an important area for future investigation.
From an educational standpoint, these findings underscore the importance of fostering diagnostic flexibility and encouraging critical engagement with symptom boundaries in the training of mental health professionals. Integrating multidimensional and culturally responsive frameworks into educational programs may further enhance diagnostic sensitivity and support more contextually informed clinical decision-making.
4.6. Directions for Future Research
Future research holds an important role in further clarifying the relationship between PTSD and psychotic disorders, particularly in light of the methodological and conceptual challenges identified in the present review. Longitudinal studies that trace symptom trajectories across diverse populations may offer deeper insight into the evolving and dynamic nature of this relationship. Additionally, the use of more standardized diagnostic criteria, alongside larger and more culturally diverse samples, may help strengthen both the validity and generalizability of future findings.
Greater attention to subgroup differences may also prove especially informative. Systematic analyzes examining how symptom expression and treatment response vary according to trauma type, developmental stage, age, or gender could provide a more differentiated understanding of PTSD presentations, dimensions that were not fully captured within the current evidence base. More broadly, advancing this field will likely depend on integrative research approaches that bring together neurobiological, psychological, and sociocultural perspectives in a more coordinated way, thereby supporting the refinement of diagnostic frameworks and intervention strategies.
Building on the present synthesis, a particularly promising direction involves the empirical examination of the hypothesis that acute trauma may disrupt neurobiological equilibrium, especially within prefrontal regulatory systems, through heightened neurochemical activation. Such disruptions may contribute to the emergence of psychotic-like experiences in PTSD, particularly in the context of complex or early-life trauma exposure. When considered in relation to dopaminergic and glutamatergic processes, this perspective suggests the possibility of partially overlapping etiological pathways linking PTSD and psychosis, while still maintaining a distinction between their underlying neuropathological profiles.
At the same time, it is important to recognize that the current evidence base remains constrained by several limitations, including relatively small sample sizes, diagnostic heterogeneity, variability in neuroimaging methodologies, and inconsistencies in the operationalization of psychotic-like symptoms. In light of these considerations, there is a clear need for sustained, multidisciplinary research efforts that integrate neurobiological and psychosocial domains. Such efforts may contribute to more precise classification approaches and support the development of increasingly individualized, trauma-informed models of care.
5. STUDY LIMITATIONS
While this systematic review provides important insights into PTSD classification and its overlap with psychotic disorders, several methodological and contextual limitations should be acknowledged. The included studies exhibited variability in design, sample size, and diagnostic criteria, resulting in heterogeneity that may limit the generalizability of the findings. In addition, methodological inconsistencies and the possibility of selective reporting may have influenced the robustness of some outcomes.
A further limitation relates to study design, as the majority of the 41 included studies employed cross-sectional or correlational approaches, which restricts causal inference regarding neurobiological alterations and clinical symptom expression. Moreover, cultural and regional differences in trauma interpretation were not consistently addressed, which may have influenced diagnostic classification and symptom reporting across contexts. Finally, although visual synthesis enhanced interpretive clarity, the absence of individual-level data precluded formal meta-analytic integration.
For methodological consistency, the review was limited to studies published between 2000 and 2024 within a PRISMA-guided framework. More recent evidence (2025) was considered contextually to reflect emerging developments but was not included in the structured synthesis. Future research would benefit from longitudinal, multi-site designs with more diverse populations to strengthen diagnostic precision and improve clinical applicability. A detailed mapping of PRISMA 2020 checklist items (1-27) is provided in File S6.
Beyond methodological constraints, real-world implementation challenges may also affect the ecological validity of psychotherapy outcomes. Limited access to trained trauma-focused clinicians, disparities in evidence-based care in low-resource or conflict-affected settings, and variability in treatment adherence among individuals with complex trauma all represent important structural barriers. These factors highlight the need for scalable, culturally adaptable, and resource-sensitive therapeutic models to support equitable access and sustained clinical benefit.
6. CHALLENGES IN RE-EVALUATING PTSD CLASSIFICATION
The present synthesis highlights several cross-cutting challenges that complicate the re-evaluation of PTSD classification, reflecting ongoing diagnostic ambiguity, methodological variability, and cultural influences. A central issue lies in the symptom overlap between PTSD and psychotic disorders, which may blur diagnostic boundaries and complicate differentiation in clinical practice. In addition, inconsistencies in the application of diagnostic systems across contexts may contribute to variability in case identification.
From a clinical perspective, this ambiguity increases the risk of misclassification, potentially leading to suboptimal treatment decisions and less effective outcomes. Neurobiological alterations associated with trauma further complicate categorical distinctions, suggesting that biological markers alone may not be sufficient for clear diagnostic separation. Cultural factors add an additional layer of complexity by shaping both symptom expression and clinical interpretation.
Within this framework, complex trauma presentations often require more individualized and context-sensitive diagnostic approaches than rigid categorical models allow. Addressing these challenges will likely depend on the development of trauma-informed, culturally responsive frameworks supported by longitudinal, multi-site research and clearer clinical guidance to improve diagnostic precision and applicability.
CONCLUSION
This review brings together neurobiological, clinical, and therapeutic evidence to provide a more integrated understanding of how PTSD may be classified. Although PTSD shares certain neurobiological and symptomatic features with psychotic disorders, such as hippocampal volume reduction, amygdala hyperactivity, and transient perceptual disturbances, these overlaps appear partial and context-dependent. Overall, the findings point toward a trauma-spectrum conceptualization, in which psychotic-like symptoms are more plausibly understood as expressions of trauma-related dysregulation rather than manifestations of primary psychosis.
Looking across the evidence, three key conclusions emerge. First, neurobiological findings show both convergence and divergence with psychosis; while some structural and functional alterations suggest partial overlap, inconsistencies across studies limit the use of neurobiology as a standalone diagnostic marker. Second, clinical evidence suggests that trauma complexity plays a central role in shaping symptom heterogeneity and diagnostic uncertainty. Third, therapeutic findings indicate that trauma-focused psychotherapy, particularly CBT and EMDR, tends to show more sustained benefits than pharmacological interventions, reinforcing the central role of psychological and trauma-related mechanisms in PTSD.
Taken as a whole, the evidence supports a dimensional model of PTSD that moves beyond categorical boundaries and instead frames the condition as a dynamic interplay between neurobiological disruption and psychological complexity. This perspective helps connect biological, clinical, and sociocultural dimensions in a way that better reflects the lived reality of trauma and may offer a more clinically meaningful foundation for refining diagnostic frameworks and supporting trauma-informed care.
AUTHORS’ CONTRIBUTIONS
The authors confirm contribution to the paper as follows: M.A.: Conceptualized the study, provided critical analysis, contributed to data interpretation, and reviewed and edited the manuscript for coherence and clarity; S.I.: Conducted the primary literature review, developed the research framework, and offered suggestions for refinement; E.E.: Assisted in the research design and contributed to refining the theoretical models and conclusions.
LIST OF ABBREVIATIONS
| PTSD | = Post-Traumatic Stress Disorder |
| PTSD-SP | = Post-Traumatic Stress Disorder With Secondary Psychotic Features |
| CBT | = Cognitive Behavioral Therapy |
| TF-CBT | = Trauma-Focused Cognitive Behavioral Therapy |
| EMDR | = Eye Movement Desensitization and Reprocessing |
| CPTSD | = Complex Post-Traumatic Stress Disorder |
| BPD | = Borderline Personality Disorder |
| PE | = Prolonged Exposure |
| CPT | = Cognitive Processing Therapy |
| SSRIS | = Selective Serotonin Reuptake Inhibitors |
| DSM-5 | = Diagnostic and Statistical Manual of Mental Disorders Fifth Edition |
| DSM-5-TR | = Diagnostic and Statistical Manual of Mental Disorders Fifth Edition, Text Revision |
| DSO | = Disturbances in Self-Organization |
| ICD-11 | = International Classification of Diseases 11th Revision |
| PRISMA | = Preferred Reporting Items for Systematic Reviews and Meta-Analyses |
| PFC | = Prefrontal Cortex |
| E-CBT | = Electronic Cognitive Behavioral Therapy |
| VA | = Veterans Affairs |
| CA-CBT | = Culturally Adapted Cognitive Behavioral Therapy |
| ROB 2.0 | = Cochrane Risk of Bias Tool (Version 2.0) |
| JBI | = Joanna Briggs Institute |
| SMD | = Standardized Mean Difference |
| OR | = Odds Ratio |
| I2 | = I-Squared Statistic; a Measure of Heterogeneity in Meta-Analyzes Expressed as a Percentage |
| K | = Number of Studies Included in a Meta-Analysis |
| R | = Statistical Computing Software Environment used for Data Analysis |
AVAILABILITY OF DATA AND MATERIALS
All the data and supportive information are provided within the article.
ACKNOWLEDGEMENTS
Declared none.